 Over the past several weeks, I’ve been immersed in educating Colorado healthcare providers on the complexities of the state’s new medical aid-in-dying law: 7 all-day programs in 6 cities attended by more than 400 professionals from all sectors and settings of healthcare plus attorneys, law enforcement, and government agencies. In the context of this experience, I was reminded—sharply—of how we still have such a long way to go with documenting and honoring patients’ choices on life-sustaining treatments, let alone responding to their requests for aid-in-dying.
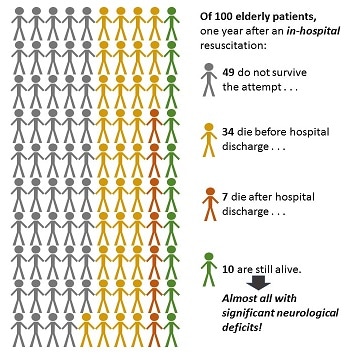
What Do We Do Now? One case study I used in the education programs involved a patient who died by medical aid in dying in California. Everything went smoothly, she died peacefully, with her family around her. She’d chosen the day after Christmas to make her exit and was not enrolled in hospice at the time. After some reminiscence and grieving, the family thought, What now? Did they need to report the death? To whom? Who would remove the body? They called the physician who had prescribed the lethal drugs; he was out for the holiday. The on-call physician said, “Um, I don’t know. I guess you should call 9-1-1.” So they did. The paramedics turned up and—without an apparent and immediately available out-of-hospital Do Not Resuscitate order (a.k.a. CPR directive) to say no—they attempted resuscitation for 30 minutes and ultimately transported the patient to the hospital where she was pronounced dead on arrival. It was ugly and traumatic for everyone. Not at all the outcome intended. I used this case study to emphasize the importance of educating family members about what to do after a medical aid-in-dying death and the importance of any patient utilizing the option having an out-of-hospital DNR/CPR Directive or POLST/MOST to avoid such traumas. Let’s be fair—first responders have strict rules about what they must do, what documentation they must have to withhold aggressive treatment, and precious little time to sort out any ambiguities. In discussing this case, a longtime fire chief attending our program explained (dryly), “When we arrive, unless there’s a DNR or obvious signs of irrevocable death – such as lividity, rigor mortis, or decapitation – we have to proceed with life-saving efforts.” Alrighty then. (I’d recommend documentation over decapitation, for the record.) Not Dead Yet? In preparing this case study, I became curious as to just what one would do if a person died at home without benefit of hospice or other attending healthcare professional. So, I turned to Google and typed, “How to report a death at home.” First in the results list was a blurb from a page on the website of a county government agency on aging issues, which advised cheerfully: If your loved one dies at home: Call the doctor or 9-1-1. If a living will or "Do Not Resuscitate" order is in place, it may sound odd, but make sure the person is dead before you call authorities. Emergency medical workers sometimes must attempt to revive a patient even if a living will or "Do Not Resuscitate" order tells them not to. If this is a concern in your situation, call the doctor for guidance before dialing 9-1-1. The bold there is mine: “must attempt to revive a patient even if . . . a ‘Do Not Resuscitate’ order tells them not to”??? (I’m not touching the living will part of this, because that’s a whole other rabbit hole.) Under what circumstances “must” an EMT break the law? I wondered. Wow, Just Wow. Picking my jaw up off the floor, I sent this little blurb out to some of my fellow travelers in the wilds of advance care planning with the subject line, “Wow, just wow.” Two stories were shared: "I do know that at least one EMS company [in my area] says rather overtly, 'No one dies in my ambulance,' and they will continue to resuscitate until the ER doc pronounces. When I told tham that was, er, illegal, they nodded and moved quietly away from the conversation." "I've met some, ah, nonconforming paramedics/EMTs. A new arrival to Colorado . . . said he worked in California and, along with—it seemed—others, disregarded DNR on a valid POLST if they felt CPR should be tried. He explained they “know better” than the patient because the patient isn't aware of future medical circumstances when the MOST/POLST is signed. To [this] point, legality doesn't matter. Doing CPR does." With these observations in the backdrop, and assuming they must be exceptions rather than a rule, I asked our fire chief at the program, “If the patient had a valid and available CPR directive, you would back off, right?” “Well, yes, then we’ll hold off,” he said. I brightened – until he finished the sentence: “But, if there’s a family member there yelling at us to do something, we generally go ahead anyway.” Note: “family member” . . . not duly-authorized-by-medical-power-of-attorney healthcare agent . . . just “family member.” Chief, love ya man, but we need to talk. Why This Is Important My graphic is based on findings from a study of long-term outcomes in elderly survivors of in-hospital attempts at resuscitation (Chan et al., New England Journal of Medicine 3/13), reported in a blog by Eric Widera in Geripal ("Outcomes of In-Hospital CPR: Not as Rosy as Some May Say"). Of 100 elderly patients who have an in-hospital cardiac arrest and resuscitation, 49 do not survive the attempt, and only 10 are still alive a year later. Of those, almost all of them will have significant neurological deficits. And that's when the resuscitation attempt is made in the hospital, with the most sophisticated equipment available, presumably within seconds of the cardiac event. Outcomes of out-of-hospital attempts are even worse: only 3 in 100 elderly persons even survive such an attempt and the neurological and physical deficits are likely to be worse. With these dire stats in mind, physicians and other healthcare providers do their best to educate older patients, especially those in nursing facilities or dealing with a serious or progressive illness at home, to execute a directive that says "NO" to CPR. What Part of DO NOT RESUSCITATE Don't We Understand? I get it if the paperwork isn't handy, but if the appropriate document refusing CPR is apparent and immediately available, there is NO defensible legal or ethical reason to ignore it, cave to the pleas of family members, think we know better, or pass the buck on to the ER. PERIOD. EVER. IN ANY STATE. I understand the messiness of real-world situations and have great empathy and respect for our first responders and other caring providers and facility staff. But it’s time we all grew some, em, spine and followed the law. When people have carefully considered, discussed, and documented their wishes in legal directives, they should have confidence that we will follow their wishes. We need to give them that confidence by backing them up: “I’m sorry [Miscellaneous Family Member or even Healthcare Agent], your mom took the trouble to complete a CPR directive. I know this is hard for you, but that’s her voice talking, and my job is to listen to it.” Can we do that?
7 Comments
|
AuthorJennifer Moore Ballentine is a longtime hospice and palliative care advocate, educator, and consultant. See About Us & Contact page for more information. ArchivesCategories |
 RSS Feed
RSS Feed