 Over the past several weeks, I’ve been immersed in educating Colorado healthcare providers on the complexities of the state’s new medical aid-in-dying law: 7 all-day programs in 6 cities attended by more than 400 professionals from all sectors and settings of healthcare plus attorneys, law enforcement, and government agencies. In the context of this experience, I was reminded—sharply—of how we still have such a long way to go with documenting and honoring patients’ choices on life-sustaining treatments, let alone responding to their requests for aid-in-dying.
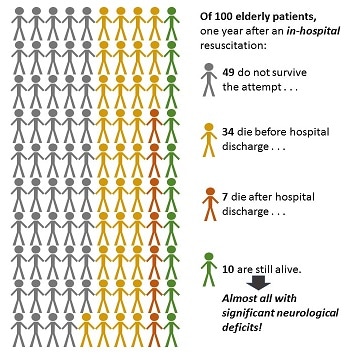
What Do We Do Now? One case study I used in the education programs involved a patient who died by medical aid in dying in California. Everything went smoothly, she died peacefully, with her family around her. She’d chosen the day after Christmas to make her exit and was not enrolled in hospice at the time. After some reminiscence and grieving, the family thought, What now? Did they need to report the death? To whom? Who would remove the body? They called the physician who had prescribed the lethal drugs; he was out for the holiday. The on-call physician said, “Um, I don’t know. I guess you should call 9-1-1.” So they did. The paramedics turned up and—without an apparent and immediately available out-of-hospital Do Not Resuscitate order (a.k.a. CPR directive) to say no—they attempted resuscitation for 30 minutes and ultimately transported the patient to the hospital where she was pronounced dead on arrival. It was ugly and traumatic for everyone. Not at all the outcome intended. I used this case study to emphasize the importance of educating family members about what to do after a medical aid-in-dying death and the importance of any patient utilizing the option having an out-of-hospital DNR/CPR Directive or POLST/MOST to avoid such traumas. Let’s be fair—first responders have strict rules about what they must do, what documentation they must have to withhold aggressive treatment, and precious little time to sort out any ambiguities. In discussing this case, a longtime fire chief attending our program explained (dryly), “When we arrive, unless there’s a DNR or obvious signs of irrevocable death – such as lividity, rigor mortis, or decapitation – we have to proceed with life-saving efforts.” Alrighty then. (I’d recommend documentation over decapitation, for the record.) Not Dead Yet? In preparing this case study, I became curious as to just what one would do if a person died at home without benefit of hospice or other attending healthcare professional. So, I turned to Google and typed, “How to report a death at home.” First in the results list was a blurb from a page on the website of a county government agency on aging issues, which advised cheerfully: If your loved one dies at home: Call the doctor or 9-1-1. If a living will or "Do Not Resuscitate" order is in place, it may sound odd, but make sure the person is dead before you call authorities. Emergency medical workers sometimes must attempt to revive a patient even if a living will or "Do Not Resuscitate" order tells them not to. If this is a concern in your situation, call the doctor for guidance before dialing 9-1-1. The bold there is mine: “must attempt to revive a patient even if . . . a ‘Do Not Resuscitate’ order tells them not to”??? (I’m not touching the living will part of this, because that’s a whole other rabbit hole.) Under what circumstances “must” an EMT break the law? I wondered. Wow, Just Wow. Picking my jaw up off the floor, I sent this little blurb out to some of my fellow travelers in the wilds of advance care planning with the subject line, “Wow, just wow.” Two stories were shared: "I do know that at least one EMS company [in my area] says rather overtly, 'No one dies in my ambulance,' and they will continue to resuscitate until the ER doc pronounces. When I told tham that was, er, illegal, they nodded and moved quietly away from the conversation." "I've met some, ah, nonconforming paramedics/EMTs. A new arrival to Colorado . . . said he worked in California and, along with—it seemed—others, disregarded DNR on a valid POLST if they felt CPR should be tried. He explained they “know better” than the patient because the patient isn't aware of future medical circumstances when the MOST/POLST is signed. To [this] point, legality doesn't matter. Doing CPR does." With these observations in the backdrop, and assuming they must be exceptions rather than a rule, I asked our fire chief at the program, “If the patient had a valid and available CPR directive, you would back off, right?” “Well, yes, then we’ll hold off,” he said. I brightened – until he finished the sentence: “But, if there’s a family member there yelling at us to do something, we generally go ahead anyway.” Note: “family member” . . . not duly-authorized-by-medical-power-of-attorney healthcare agent . . . just “family member.” Chief, love ya man, but we need to talk. Why This Is Important My graphic is based on findings from a study of long-term outcomes in elderly survivors of in-hospital attempts at resuscitation (Chan et al., New England Journal of Medicine 3/13), reported in a blog by Eric Widera in Geripal ("Outcomes of In-Hospital CPR: Not as Rosy as Some May Say"). Of 100 elderly patients who have an in-hospital cardiac arrest and resuscitation, 49 do not survive the attempt, and only 10 are still alive a year later. Of those, almost all of them will have significant neurological deficits. And that's when the resuscitation attempt is made in the hospital, with the most sophisticated equipment available, presumably within seconds of the cardiac event. Outcomes of out-of-hospital attempts are even worse: only 3 in 100 elderly persons even survive such an attempt and the neurological and physical deficits are likely to be worse. With these dire stats in mind, physicians and other healthcare providers do their best to educate older patients, especially those in nursing facilities or dealing with a serious or progressive illness at home, to execute a directive that says "NO" to CPR. What Part of DO NOT RESUSCITATE Don't We Understand? I get it if the paperwork isn't handy, but if the appropriate document refusing CPR is apparent and immediately available, there is NO defensible legal or ethical reason to ignore it, cave to the pleas of family members, think we know better, or pass the buck on to the ER. PERIOD. EVER. IN ANY STATE. I understand the messiness of real-world situations and have great empathy and respect for our first responders and other caring providers and facility staff. But it’s time we all grew some, em, spine and followed the law. When people have carefully considered, discussed, and documented their wishes in legal directives, they should have confidence that we will follow their wishes. We need to give them that confidence by backing them up: “I’m sorry [Miscellaneous Family Member or even Healthcare Agent], your mom took the trouble to complete a CPR directive. I know this is hard for you, but that’s her voice talking, and my job is to listen to it.” Can we do that?
7 Comments
The dust is still settling from the election—we have some state-level results to report and some speculation about what the new administration will mean for healthcare nationally.
Overall, the measures we identified as related to palliative and end-of-life care before the election fared well: 7 passed; 2 rejected; 1 removed from the ballot prior to the election due to invalid signatures (details below). Notably, Arkansas, Florida, North Dakota, and Montana all approved medical marijuana, bringing the total to 20 states. (At the same time, Maine, Massachusetts, Nevada, and California approved recreational marijuana.) The physician-assisted death proposition passed in Colorado, which joins Oregon, Washington, Vermont, and California in offering the option. Voters there, however, overwhelmingly rejected an amendment to establish a state healthcare system, and Montana voters rejected a bond measure to establish a state authority to make research grants to develop therapies and cures for brain injuries and neurological diseases. With the surprise win for Donald Trump of the presidency, healthcare in general is headed for a time of uncertainty and turmoil. One of Trump’s signature campaign issues was to repeal and replace Obamacare, although specifics from him on the replacement have been thin. Just over the past several days, news reports have suggested that Trump is considering trying to preserve key features of Obamacare, while others suggest that the law will be repealed “on Inauguration Day.” Even in the case of a wholesale repeal pundit comments offer reassurance that effects would be phased in and unlikely to impact beneficiaries of subsidized policies until 2018. This “repeal but delay” scenario seems to be gaining steam, though not without its own chaotic effects. In a recent presentation at the Hospital Quality Conference in San Diego, healthcare “futurist” Ian Morrison, PhD, offered predictions for what changes might be in the offing under a Trump administration, including major structural changes in the Affordable Care Act (and likely a changed name), an end to mandated participation by individuals and corporations, elimination or reduction of the tax on so-called “Cadillac” health plans, establishment of state-administered high-risk pools for people with pre-existing conditions, reduced federal subsidies for middle- and low-income and Medicaid beneficiaries, more state discretion and control over Medicaid spending (and thus more variability from state to state in benefits and services), and less regulation of insurance. Biggest implications for hospice in these changes is potential for Medicaid hospice benefits to be reduced or cut in states exercising additional discretion over spending and services. Of course, there’s a great deal more to Obamacare, and healthcare reform generally, than “just” the insurance exchanges and Medicaid expansion, which might more directly affect palliative and end-of-life care. A healthcare policy announcement Thursday on Trump’s transition website www.greatagain.gov has some in the palliative care community concerned that Trump policies may result in a roll-back of support for advance care planning, advance directives, and patient choice in decisions around life-sustaining treatment—possibly even a resurgence of the “death panels” rhetoric and resistance. Another concern is the potential dismantling of Medicare as a system and its currently robust benefits, including hospice. While Trump’s policy statements are vague, Paul Ryan’s conservative agenda is much more specific, and likely to significantly inform reform legislation. Although hospice is not mentioned once in the detailed policy paper, Ryan’s A Better Way agenda includes expanding Medicare Advantage programs, repealing the Medicare Independent Payment Advisory Board, combining Medicare Parts A and B, and abolishing the Center for Medicare and Medicaid Innovation (CMMI). Among many other programs, the CMMI administers the Medicare Care Choices Model, allowing concurrent curative and palliative care, which has – or had – another four years to run. Ryan’s agenda also suggests largely or wholly privatizing Medicare, moving away from direct payment for services and more toward premium support, or significantly reducing coverage. Policies may be significantly shaped, too, by who is appointed as Secretary of Health and Human Services. In the running right now: Newt Gingrich (House Speaker in the 1990s), Bobby Jindal (former Louisiana Governor and presidential candidate), Rick Scott (current Florida Governor), and Richard Bagger (VP Celgene Corporation and former New Jersey State Senator). Ben Carson (neurosurgeon and presidential candidate) was under consideration but has taken himself out of the running. All these candidates have at least some healthcare administration or policy development in their backgrounds: Gingrich, after leaving the House, founded and chaired the Center for Health Transformation. Bagger, an attorney, has served as house counsel for Horizon Blue Cross Blue Shield of NJ and lobbyist for Pfizer. Celgene is a global biopharmaceutical company developing drugs and treatments for cancer and immune system disorders. In his mid-twenties, Bobby Jindal served as Secretary of the Louisiana Department of Health and Hospitals, and later, in the George W. Bush administration, as advisor to the U.S. Secretary of Health and Human Services. In the 1990s, Rick Scott was a cofounder of Columbia Hospital Corporation, which later merged with Hospital Corporation of America to form the largest for-profit health care company in the country. A podcast for members from the National Hospice and Palliative Care Organization last week, however, took the view that with the new administration, Congress, and HHS Secretary, impacts on hospice were likely to be more in the nature of a “gear shift” than the “seismic shift” others are anticipating. Hospice, they noted, enjoys bipartisan support and that its “friends and champions” of both parties are “going to be back” next year. Even with anticipated changes in the Secretary of Health and Human Service and among some appointees to CMS, many longtime career personnel will remain in place. NHPCO’s message? Keep calm and carry on. Finally, expansion of physician aid in dying laws may well hit speed bumps, because of the changed tone at the top and because of significant shifts to the right in state governments. As a result of last week’s election, four states shifted to full control (both legislative chambers and the Governor’s office) by Republicans, bringing the total to 24. In another 7 states, Republicans control both chambers of the legislature, though not the Governor’s office. While physician aid in dying has support from both parties, Republican-controlled legislatures and Governors have generally been less friendly to the issue. That said, Compassion & Choices has announced plans to pursue expansion, targeting Maryland, Minnesota, and New York. Results of Ballot measures: Arkansas Issue 6, Arkansas Medical Marijuana Amendment of 2016 – PASSED (53–47%) Issue 7, Arkansas Medical Cannabis Statute – REMOVED FROM BALLOT 10/27/16 DUE TO INVALID PETITION SIGNATURES. California Proposition 56, Tobacco Tax – Increase – PASSED (63–37%) Colorado Amendment 69, State Healthcare System – REJECTED (79–21%) Proposition 106, Colorado End of Life Options Act – PASSED (65–35%) Florida Amendment 2, Medical Marijuana Legalization – PASSED (71–29%) Montana I-181, Bonds to Fund Biomedical Research Authority – REJECTED (58–42%) I-182, Medical Marijuana Initiative – PASSED (58–42%) Nevada Question 4, Medical Equipment Sales Tax Exemption Initiative (a.k.a. Medical Patient Tax Relief Act) – PASSED (72–28%) North Dakota Measure 5, Medical Marijuana Legalization Initiative (a.k.a. North Dakota Compassionate Care Act) – PASSED (64–38%) Palliative Care on the Ballot: A Roundup of Issues Related to Palliative and End-of-Life Care on Statewide Ballots, November 8, 2016
In all the contention leading to the November 8th election, the topic of healthcare has not been much discussed and palliative care not at all. In several states, however, important issues relevant to palliative and end-of-life care are up for consideration. Medical marijuana is big this year, on the ballot in four states (and recreational marijuana in five). Physician-assisted death is on the ballot in Colorado, having failed to pass the state’s legislature in 2015 and 2016. Colorado also has a single-payer state-run health payment system on the ballot, and other states are raising taxes on tobacco, removing them from medical equipment, and floating bonds to fund research. And North Dakota is giving "Compassionate Care" a whole new meaning!! Here’s a roundup; links will take you to specific language and pro/con discussions: Arkansas Issue 6, Arkansas Medical Marijuana Amendment of 2016, and Issue 7, Arkansas Medical Cannabis Statute: to legalize medical marijuana. The two measures differ in details and in implementation: Issue 6 as a state constitutional amendment and Issue 7 as an initiated state statute. If both pass, the one with the larger number of votes will take effect. Issue 6 charges the state Department of Health to define patient eligibility and health conditions that qualify for medical marijuana use. Issue 7 details specific conditions and symptoms, including intractable pain. California Proposition 56, Tobacco Tax Increase: increases tax on tobacco and tobacco products, including electronic cigarettes, to fund various initiatives including primary care and emergency physician training; cancer, cardiovascular and lung disease research; and to continue funding for other tobacco tax-supported programs. Colorado Amendment 69, State Healthcare System: Authorizes a state tax increase, assessed from payroll and income taxes, totaling $25 billion to establish a state-administered healthcare payment system (ColoradoCare) to fund, as primary or secondary payment source, a defined set of healthcare services for all Colorado state residents. Services include “palliative and end-of-life care.” Relationships between ColoradoCare and other payers including Medicare and Medicaid are detailed in the full text of the amendment. Proposition 106, Colorado End of Life Options Act: Creates statute establishing a legal framework under which competent, terminally ill patients with a prognosis of 6 months or less may request and receive a prescription for lethal medications for the purpose of ending their lives. Process steps are similar, though not identical, to similar statutes in Oregon and California. Florida Amendment 2, Medical Marijuana Legalization: a state constitutional amendment to allow physicians to prescribe marijuana to eligible patients with specific conditions, including cancer, ALS, HIV/AIDS, Parkinson’s, and others. Montana I-181, Bonds to Fund Biomedical Research Authority: establishes a state authority to oversee and review grant applications to promote development of therapies and cures for brain diseases and injuries and mental illnesses, including Alzheimer’s, Parkinson’s, brain cancer, dementia, traumatic brain injury and stroke by Montana biomedical research organizations. I-182, Medical Marijuana Initiative: amends an initiative approved by voters in 2004, which had been hobbled by a repeal attempt and veto of the repeal. Allows prescription of marijuana to patients with debilitating medical conditions, including cancer, HIV/AIDS, and others, that produce wasting, chronic pain, nausea, seizures, or other conditions defined by the state. This measure includes PTSD in the qualifying conditions. Nevada Question 4, Medical Equipment Sales Tax Exemption Initiative (a.k.a. Medical Patient Tax Relief Act): state constitutional amendment to exempt from sales and use tax durable medical equipment, oxygen delivery equipment, and mobility-enhancing equipment prescribed by licensed health care provider. North Dakota Measure 5, Medical Marijuana Legalization Initiative (a.k.a. North Dakota Compassionate Care Act): creates state statute to legalize use of marijuana by eligible patients with debilitating medical conditions, including cancer, AIDS, hepatitis C, ALS, and others. |
AuthorJennifer Moore Ballentine is a longtime hospice and palliative care advocate, educator, and consultant. See About Us & Contact page for more information. ArchivesCategories |
 RSS Feed
RSS Feed